
Rethinking Chronic Prostatitis: When It’s Not Just the Prostate
Chronic prostatitis is one of the most common urologic diagnoses in men, yet it is also one of the most misunderstood, mistreated, and misdiagnosed.
Many men are told they have “prostatitis,” prescribed antibiotics, and sent on their way. But what happens when symptoms persist… despite normal labs, negative cultures, and multiple rounds of treatment?
This is where the conversation needs to shift.
Understanding Chronic Prostatitis vs. CPPS
Chronic prostatitis is often used as an umbrella term, but clinically, there are different categories.
The most common form is Chronic Pelvic Pain Syndrome, or CPPS. CPPS is marked by pelvic pain lasting longer than 3 months, having no identifiable infection or clear pathology, and which is often accompanied by urinary and/or sexual symptoms.
In fact, up to 90–95% of men diagnosed with “chronic prostatitis” fall into this category, meaning the condition is non-bacterial in nature (Pendegast et al., 2025; Polackwich & Shoskes, 2016).
So why do symptoms persist?
If it’s not infection, what is it?
A growing body of clinical evidence points toward a more comprehensive explanation: Chronic pelvic pain is often driven by pelvic floor neuromuscular dysfunction, not just the prostate.
“Pelvic floor neuromuscular dysfunction” can be understood as pelvic floor hypertonicity (increased resting muscle tension), neuromuscular coordination deficits (how smoothly the body can sequence muscle contraction), and nervous system sensitization (discussed below).
CPPS is multifactorial. Muscles, nerves, connective tissue — even stress and psychosocial factors — all play a role in the symptoms of CPPS. Let’s look at these factors in more detail.
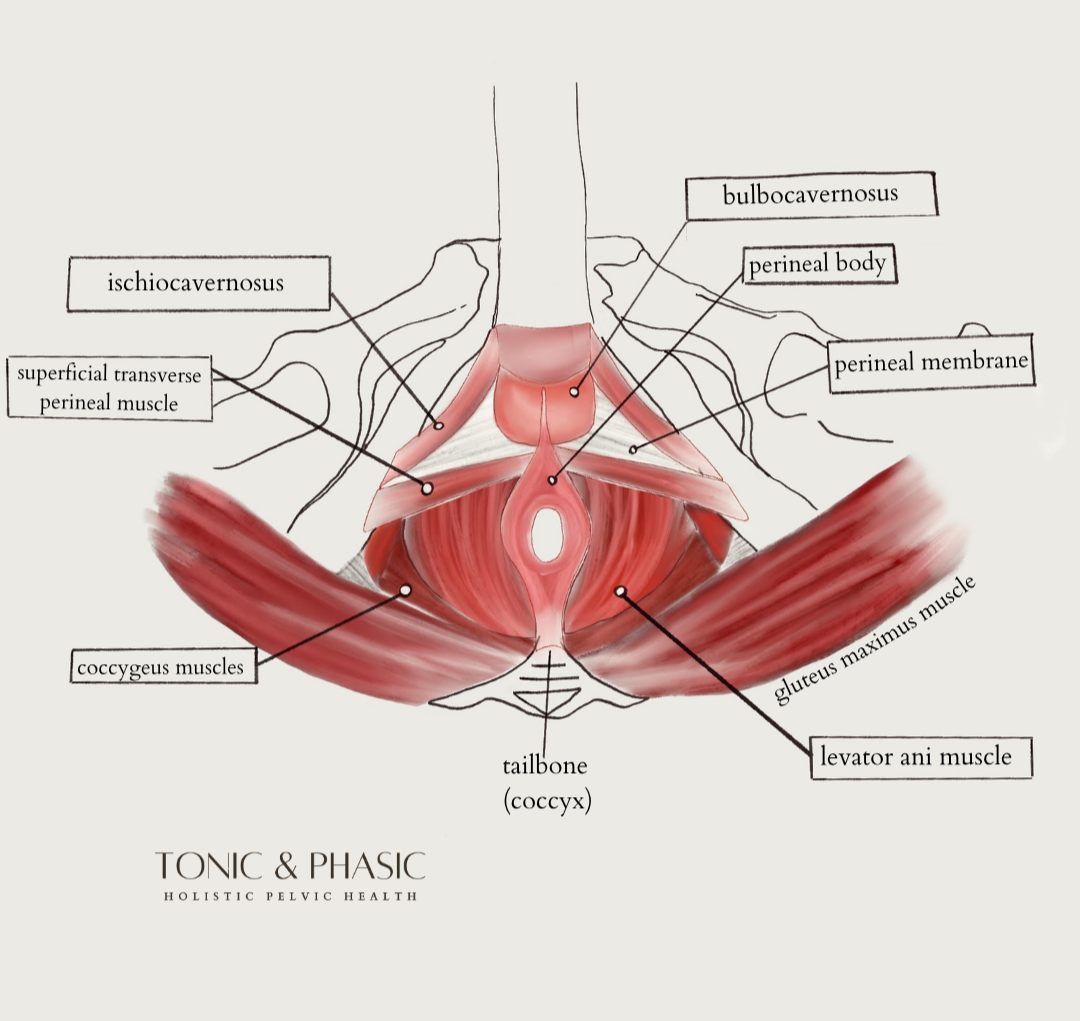
Muscles
Commonly involved muscles include:
The levator ani group (pubococcygeus, puborectalis, iliococcygeus)
Obturator internus
Urogenital diaphragm
Superficial perineal muscles (bulbocavernosus, ischiocavernosus
Like any other, these muscles can develop increased resting tone (hypertonicity), trigger points, or impaired relaxation. But because of their proximity to the pelvic organs, all of these developments may refer pain to the prostate, penis, testes or perineum; and/or contribute to urinary urgency, hesitancy, or burning.
Nerves
Key neural structures include the pudendal nerve, the obturator nerve, and contributions from the lumbosacral nerve roots (T12-L2, S2-S4). Dysfunction in these regions can range from nerve irritation to increased fight-or-flight activity (sympathetic nervous system); and often alters signaling between the pelvic organs and muscles.
These changes can amplify pain and contribute to persistent symptom patterns (more below).
Connective Tissue
Connective tissue is a factor you may not think about when considering the pelvic region. But our fascia and ligaments can greatly contribute to symptoms of CPPS. The periprostatic fascia, urogenital fascia, scarpa’s fascia, and sacrotuberous, sacrospinous, and inguinal ligaments are all structures worth considering when it comes to CPPS.
Connective tissue in the pelvis connects the pelvic floor muscles to the hips, low back, and abdominal wall. For multiple reasons, these structures can develop restrictions or decreased mobility and irritate the surrounding nerves, contribute to referred pain, and alter mobility of the pelvic region.
Stress and Psychosocial Factors
We’ve mentioned the nerves of the pelvic region. But how do stress and psychosocial factors come communicating through the nerves? Chronic stress or anxiety, high-pressure work environments and prolonged sitting, a history of injury, surgery, or medical procedures; sleep disturbances and fatigue, even fear-based movement patterns or symptom-related anxiety all influence our central nervous system.
These factors can easily lead to increased muscle tone in the pelvic floor, heightened pain sensitivity (central sensitization) and a persistent pain-tension cycle.
Because these systems are so closely interconnected, dysfunction rarely exists in isolation—which is why a comprehensive, systems-based approach is essential for effective treatment.
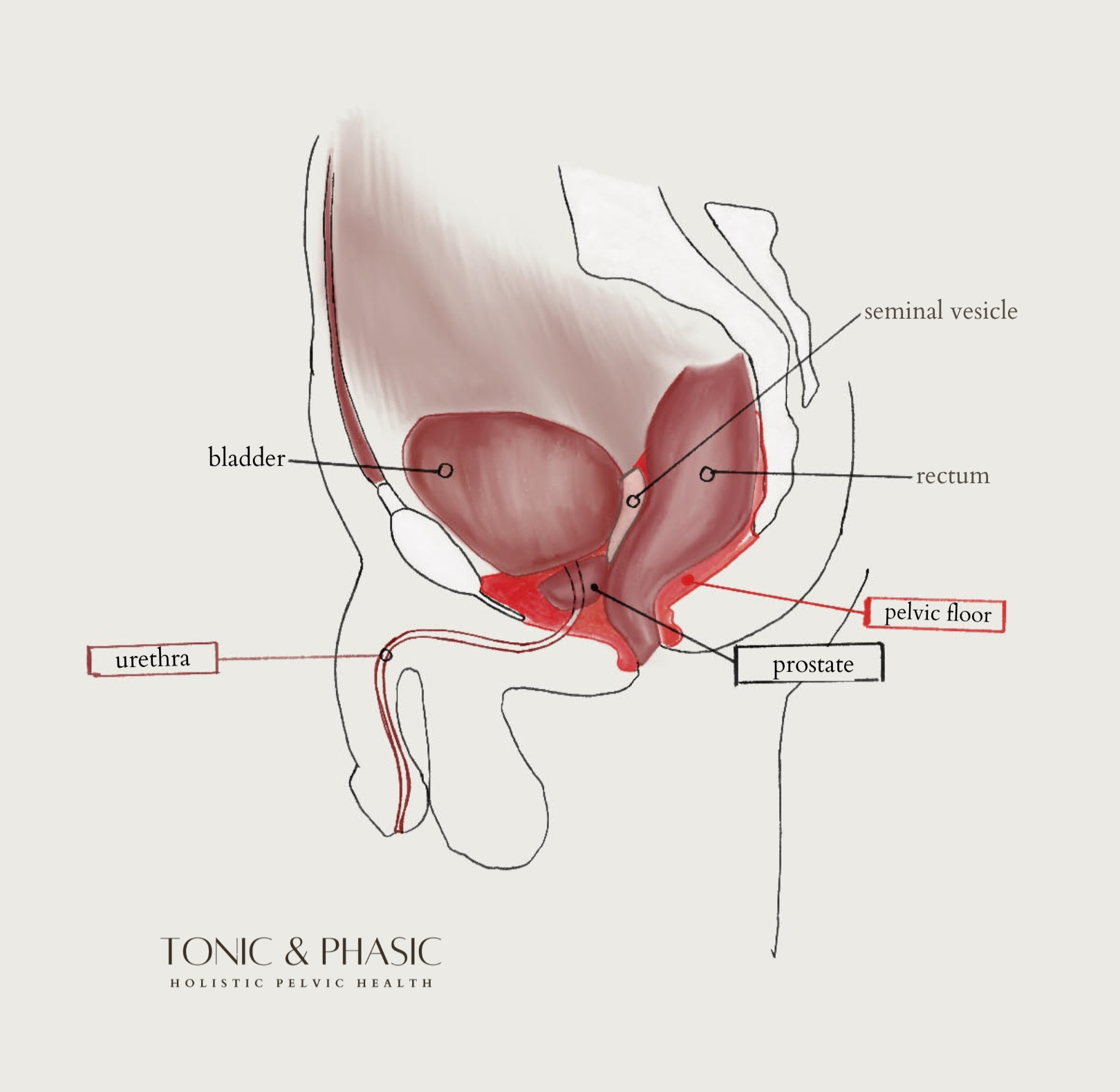
Why It Can Feel Like a “Prostate Problem”
The symptoms are real and they often feel very prostate-specific:
Deep pelvic or perineal pain
Testicular or penile discomfort
Pain with or after ejaculation
Urinary urgency, frequency, or burning
So why does it feel like it’s coming from the prostate? Let’s get clinical…
1. Referred Pain and shared Pathways
The pelvic floor muscles, bladder, and prostate share overlapping nerve pathways, creating what we call visceral-somatic “cross-talk,” and referred pain patterns. With referred pain patterns, the body refers pain to other systems. Muscle tension can feel like organ pain. Nerve irritation can mimic inflammation.
This is why many men experience a cluster of urinary, sexual, and pain symptoms simultaneously.
2. The Pain-Tension-Sensitization Cycle
Let’s talk about Central Sensitization, one of the main factors in persistent symptoms.
It often follows this pattern:
Initial trigger (infection, stress, injury, etc.)
Pelvic floor muscle tightening or guarding
Reduced blood flow and increased nerve sensitivity due to muscle tension
Increase in pain
Muscles tighten further in response
It becomes a positive feedback loop. Over time, the nervous system becomes more reactive, this is known as central sensitization.
The result? Symptoms last longer, flare more easily, and feel disproportionate to what is found during testing.
Common Clinical Patterns We See
Men with CPPS often report that symptoms worsen with sitting. We also see patients who report pain after ejaculation, fluctuation based on stress or activity, temporary relief with movement, stretching, or bowel movements, and repeated negative testing despite persistent symptoms.
As Pelvic Floor Therapists, these patterns are strong clinical indicators that the pelvic floor and surrounding musculoskeletal system are involved, rather than a recurrent infection (especially with repeat negative testing).
Traditional Treatment vs Pelvic Floor Therapy
When treated as purely urologic, CPPS is often addressed with antibiotics, alpha blockers, and anti-inflammatories. These may be appropriate in certain cases; but these methods do not treat recurrent muscle tension and nervous system dysregulation. With this purely urologic approach, patients will often experience temporary relief with the return of symptoms; and repeat treatment becomes a feedback loop of its own.
Where Pelvic Floor Physical Therapy Fits In
Pelvic floor therapy provides a targeted, systems-based approach to treating CPPS. Proper treatment addresses all systems discussed above, considering muscle tone, nerve mobility, breathing, pressure mechanics, movement patterns, and stress and nervous system regulation.
The pelvic floor is deeply connected to surrounding systems—and must be treated as such. When just one factor is considered, treatment is not nearly as effective.
What Treatment May Look Like
A typical plan of care is individualized but often includes manual therapy, neuromuscular retraining, nervous system regulation, and movement and functional integration. Let’s look at each facet of care.
Manual Therapy
Internal and external muscle release of the pelvic floor muscles
Myofascial and connective tissue techniques
Neuromuscular Retraining
Improving coordination between diaphragm and pelvic floor
Restoring the ability to fully relax muscles
Nervous System Regulation
Pain science education
Breathwork and down-training strategies
Movement and Functional Integration
Addressing contributing factors from the hips, spine, and core
Gradual return to activity
These facets come together to form an effective multimodal approach. And often, combining physical therapy with medical care has been shown to significantly improve outcomes in men with chronic pelvic pain.
When to Consider Pelvic Floor Physical Therapy
There are a few things to look out for when you’re experiencing chronic pelvic pain. You may benefit from pelvic floor therapy if you notice any of the following:
Pelvic pain lasting longer than one month
Negative urine cultures or imaging
Pain with sitting, stress, or ejaculation
Persistent urinary symptoms without infection
Associated low back, hip, or abdominal tension
The Takeaway
Chronic prostatitis is not always about the prostate. In fact, for many men, it reflects a pelvic floor and nervous system condition, one that is highly treatable when approached from a comprehensive, multidisciplinary perspective.
When we expand the conversation beyond infection, we open the door to more accurate diagnoses, more effective treatment, and more sustainable recovery.
Book a free discovery call today to learn more about your anatomy, inquire about our services, and get started on your treatment plan.
Citations:
Masterson, T. A., Masterson, J. M., Azzinaro, J., Manderson, L., Swain, S., & Ramasamy, R. (2017). Comprehensive pelvic floor physical therapy program for men with idiopathic chronic pelvic pain syndrome: A prospective study. Translational Andrology and Urology, 6(5), 910–915.
Pendegast, H. J., Leslie, S. W., & Rosario, D. J. (2025). Chronic Prostatitis and Chronic Pelvic Pain Syndrome in Men. StatPearls Publishing
Polackwich, A. S., & Shoskes, D. A. (2016). Chronic prostatitis/chronic pelvic pain syndrome: A review of evaluation and therapy. Prostate Cancer and Prostatic Diseases, 19(2), 132–138.
Medical Disclaimer: This content is intended for educational purposes only and does not constitute medical advice. If you are experiencing symptoms, please consult with a qualified healthcare provider or pelvic floor physical therapist for an individualized evaluation and plan of care.