
Dysmenorrhea: What’s Normal, What’s Not, and How Pelvic Floor PT Helps
Counting down the days. Canceling plans. Staying in bed.
Sharp, stabbing cramps. Low back pain. Migraines. Nausea. Sometimes vomiting.
For some people, their period arrives quietly, almost unnoticed. For others, symptoms start days (or even a week) before bleeding begins and disrupt daily life entirely.
Painful periods, clinically known as dysmenorrhea, are often normalized. Missing school or work, relying on NSAIDs just to function, or feeling temporarily bedridden is brushed off as “just part of having a period.” But debilitating pain is not something you should have to push through.
To understand why period pain happens, and how pelvic floor physical therapy can help, we need to start with the menstrual cycle itself.
Menstrual Cycle 101: The Communication Loop
Each month, your body moves through natural ebbs and flows, physically, mentally, and hormonally. This happens because of a highly coordinated communication system between the brain and the ovaries.
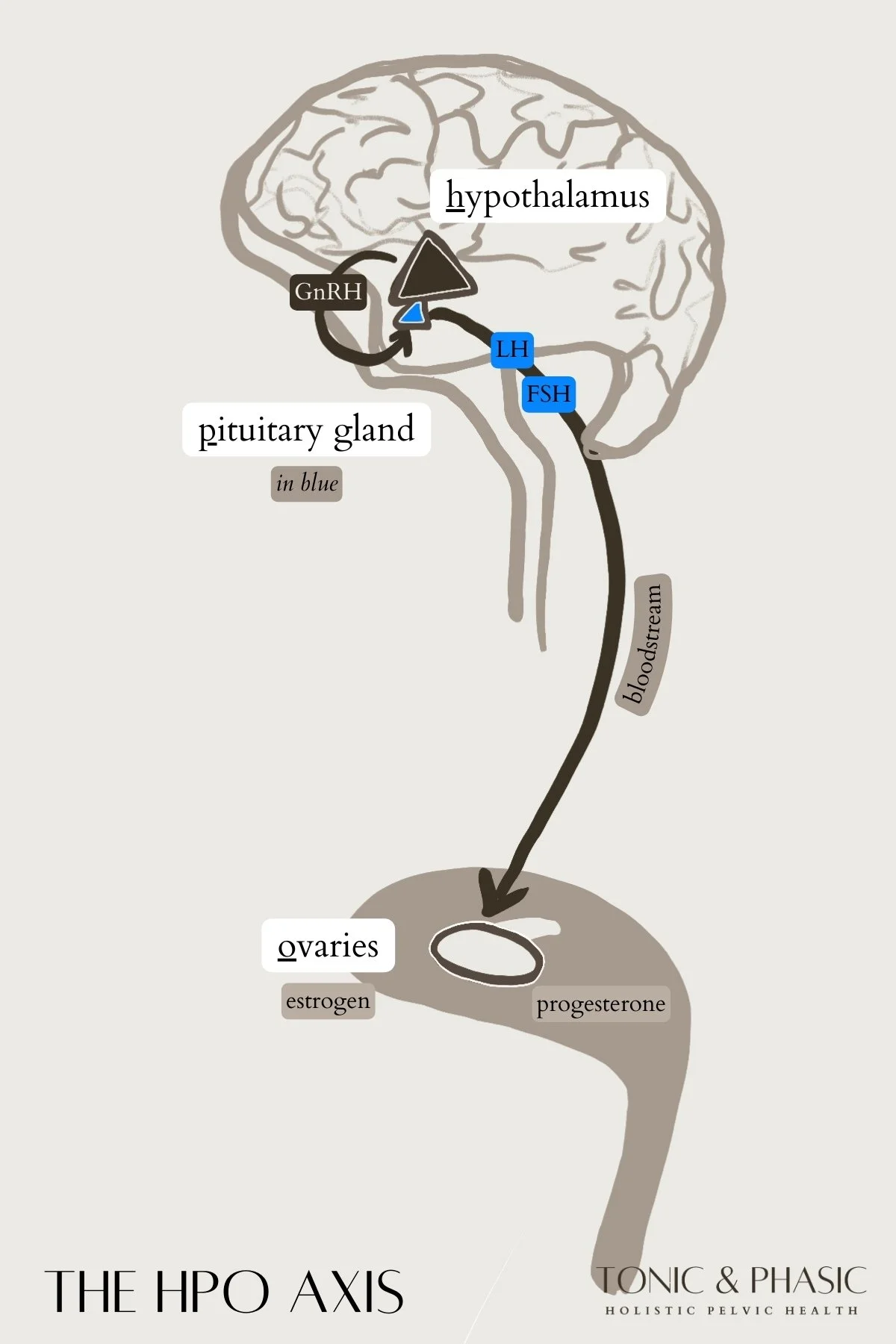
This system is called the Hypothalamic–Pituitary–Ovarian (HPO) Axis.
Here’s the big picture:
The hypothalamus signals the pituitary
The pituitary signals the ovaries
Hormones like GnRH, FSH, LH, estrogen, and progesterone rise and fall in response
When this communication is smooth, the cycle flows beautifully. But when signaling is disrupted, through stress, inflammation, hormone imbalances, or nervous system overload, symptoms can show up. Period pain is one of the most common signals that the HPO Axis has been disrupted.
Ovarian Cycle vs. Uterine Cycle (And Why It Matters)
Menstrual cycles naturally vary from person to person.
Not everyone ovulates on Day 14—in fact, ovulation can occur anywhere between Days 10 and 21. Because ovulation timing differs, overall cycle length differs too. A typical cycle can range from 21 to 35 days and still be considered within the normal spectrum, though we often see the “sweet spot” land between 26 and 32 days. A menstrual cycle begins on the first day of bleeding and ends the day before the next bleed begins. That full span of time is one complete menstrual cycle.
The menstrual cycle is often talked about in fragments, labeled with different names, and explained in ways that can feel confusing. Yet behind all of those terms is a beautifully orchestrated process with a rich history and a clear rhythm. Understanding where these phases come from, and how they work together, can completely change the way we relate to our bodies. Let’s start with a simple breakdown of the types of cycles, along with a bit of context on how we came to understand it in the first place.
The Ovarian Cycle
What’s happening in the ovaries:
The ovarian cycle is driven by communication between the brain and the ovaries, guiding hormone shifts that prepare an egg for release each month.
Follicular Phase: This phase begins on Day 1 of bleeding. Several follicles, each containing an immature egg, start to mature under the influence of follicle-stimulating hormone (FSH). While many follicles begin this process, typically only one becomes dominant. During this time, estrogen levels gradually rise, influencing energy, focus, and tissue health throughout the body.
Ovulatory Phase: Ovulation occurs when a surge of luteinizing hormone (LH) signals the ovary to release the mature egg. This egg then travels into the fallopian tube, where fertilization may occur. Ovulation is a brief but powerful event, often associated with increased cervical fluid, heightened body awareness, and subtle shifts in sensation or pelvic pressure.
Luteal Phase: After ovulation, the follicle transforms into the corpus luteum, a temporary endocrine structure that produces progesterone. Progesterone plays a critical role in supporting potential pregnancy, calming the nervous system, and stabilizing tissues. If pregnancy does not occur, progesterone levels eventually fall, signaling the body to begin the next cycle.
The Uterine Cycle
What’s happening in the uterus
While the ovaries are managing hormone production and egg release, the uterus is responding to those hormonal signals by preparing its lining.
Menstrual Phase: This is the phase we recognize as a period. The uterine lining sheds, resulting in bleeding. This process is an active inflammatory and healing phase that can influence pain sensitivity, muscle tension, and fatigue.
Proliferative Phase: As estrogen rises, the uterine lining begins to rebuild and thicken. Blood vessels form, tissue regenerates, and the uterus becomes more receptive. This phase often coincides with increased energy, improved tissue elasticity, and a greater tolerance for physical and mental stress.
Secretory Phase: Guided by progesterone, the uterine lining becomes more nutrient-dense and organized, preparing for possible implantation. If implantation does not occur, hormone levels eventually decline, and the lining prepares to shed once again.
Bringing It All Together
The ovarian cycle and the uterine cycle are happeningat the same time, constantly communicating through hormones and feedback loops. This overlap is where we get the term the menstrual cycle, a combined view that brings both cycles into one cohesive framework.
When we talk about the menstrual cycle as we commonly know it, we’re really describing four integrated phases that reflect what’s happening in both the ovaries and the uterus: menstrual, follicular, ovulatory, and luteal. Each phase represents a unique hormonal environment that influences not only bleeding and ovulation, but also pain perception, pelvic floor tone, energy levels, and overall body awareness.
By understanding the menstrual cycle in this complete way, rather than as isolated events, we can begin to make sense of symptoms that may otherwise feel random or frustrating.
Let’s break down the menstrual cycle as we know it, in full.
The Four Phases of the Menstrual Cycle
1. Menstrual Phase
This phase reflects the shedding of the uterine lining as estrogen and progesterone drop. It is an inflammatory and restorative phase, and the body is doing real work here.
Days 1–7 (ideally 3–6 days)
Day 1 is defined as the first day of your heaviest flow, not spotting.
What’s typically considered normal:
Crimson red blood
Moderate, steady flow (changing every 3-4 hours)
Mild cramping (prostaglandins help the uterus contract and shed tissue)
Signs something may be off:
Severe or debilitating pain (dysmenorrhea)
Needing to change protection after less than 2 hours
Constant leaking or flooding
Very light, dry, or absent bleeding
Pelvic PT insight: Excessive cramping is not just “in your head” or something to tolerate. It may be linked to pelvic floor muscle tension, impaired uterine mobility, restricted blood flow, fascial restrictions, or an upregulated nervous system that amplifies pain signals.
Support tip: Warmth can be incredibly therapeutic during this phase. Keeping the uterus warm with soups, broths, teas, warming spices, heat packs, or infrared light may help improve circulation, ease muscle tension, and reduce pain.
2. Follicular Phase
As we learned previously the follicular phase technically begins on Day 1 of bleeding, however under this menstrual cycle breakdown we often consider the follicular phase after bleeding has stopped.
The primary goal of this phase is to nourish a dominant follicle so a healthy egg can mature. Estrogen begins to rise, supporting tissue repair, energy, and cognitive clarity.
Days 1–14 (commonly 10–17 days)
Pelvic PT + hormone support insight: Ovarian signaling and hormone delivery can be interfered by abdominal or pelvic fascial restrictions, impaired blood flow, pelvic congestion, and poor lymphatic drainage.Often, these physical factors are overlooked, but can all meaningfully influence cycle health.
Support tip: Nutrients that support mitochondrial health, such as CoQ10 (or ubiquinol) and antioxidants, may help support egg quality. Movement during this phase supports blood flow and lymphatic drainage.
3. Ovulatory Phase
~24 hour phase (with a ~6-day fertile window)
Ovulation itself is brief, but because sperm can survive in the reproductive tract for up to five days, this creates a fertile window of about a week.
This phase is marked by a surge in luteinizing hormone (LH), leading to the release of an egg from the ovary.
Tracking tips:
LH strips can help predict ovulation, as LH typically rises8–36 hours before ovulation
Basal body temperature confirms ovulation after it has already occurred
Pelvic PT insight: Restricted pelvic tissue mobility, fibroids, cervical tension, or fascial tightness may contribute to pain with ovulation, pelvic pressure, or mid-cycle spotting. Ovulation should not feel sharp or debilitating.
4. Luteal Phase
Days 17–28 (ideally 12–15 days)
The luteal phase begins after ovulation and is driven by progesterone. This phase prepares the body for either implantation or the return of menstruation.
Progesterone has a calming effect on the nervous system and supports tissue stability, sleep, and digestion. When this phase is too short or symptoms are intense, it may signal that the body is under stress.
Signs something may be off:
Short luteal phases
Significant PMS or PMDD symptoms
Anxiety, sleep disruption, or breast tenderness
Support tip: Nutrients such as vitamin B6, vitamin C, and herbs like vitex, are supportive of progesterone if your luteal phase is shorter than 10 days.
Try our Free Handout: Cycle Intuition: Hormone Supporting Swaps
What Causes Painful Periods?
Painful periods, or dysmenorrhea, are rarely caused by a single factor.
Instead, they’re often the result of multiple systems interacting at once, hormonal, musculoskeletal, nervous, and visceral.
Several contributors may play a role, including:
Elevated prostaglandins, which increase uterine contractions
Inflammation that heightens pain sensitivity
Poor detoxification or lymphatic drainage, leading to tissue congestion
Pelvic floor muscle tension or guarding
Fascial restrictions or adhesions that limit tissue mobility
Structural factors such as fibroids, cysts, or polyps
Restricted cervical or uterine mobility
Hormone imbalances affecting cycle regulation
Nervous system upregulation, where the body stays in a heightened stress response
Conditions such as endometriosis
Poor hydration and circulation, which can worsen cramping and ischemic pain
Key takeaway: Period pain is rarely “just hormonal.” The way the muscles, fascia, organs, hormones, and nervous system communicate with one another all influence how pain is experienced during the menstrual cycle.
How Pelvic Floor Physical Therapy Helps Dysmenorrhea
Pelvic floor physical therapy doesn’t just focus on symptom relief, it works to address the root contributors of period pain by supporting the way the body moves, regulates, and responds throughout the menstrual cycle.
Pelvic floor PT may help by:
Releasing pelvic floor, abdominal, and hip tension that can restrict movement and blood flow
Improving uterine and pelvic organ mobility, allowing the uterus to contract and shed more efficiently
Supporting lymphatic and circulatory flow, reducing congestion and inflammatory buildup
Downregulating the nervous system, helping the body shift out of a heightened pain response
Reducing persistent pain signaling patterns that amplify cramping over time
Addressing posture, breathing mechanics, and pressure management, which directly influence pelvic tension and intra-abdominal pressure
At Tonic & Phasic, pelvic floor physical therapy is often paired with hormone coaching and integrative support to create a more complete and personalized approach to care. This may include cycle tracking and interpretation to better understand hormonal patterns, herbal support to help ease symptoms, and lifestyle and nutrition coaching to support hormone balance and tissue health. We also provide endometriosis screening, and when appropriate, collaborate with expert endometriosis surgeons to ensure timely, comprehensive care.
Where Do I Start?
When period pain has been dismissed, minimized, or normalized for years, it can feel hard to know where to begin. Pelvic floor physical therapy is often a powerful starting point, especially when you’re looking for answers that go beyond “this is just how your body is.”
Here are a few supportive ways to begin reconnecting with your cycle and your body:
Educate yourself. Reading books like Period Repair Manual, Hormone Intelligence, Roar, or Taking Charge of Your Fertility can help you better understand hormonal patterns, cycle physiology, and what your body may be asking for.
Start tracking your cycle. Apps like Kindara or Natural Cycles (20% off code) make it easy to log bleeding, symptoms, and fertile windows. Tracking helps you notice patterns, understand your phases, and share accurate information with your provider.
Gather data. Consider obtaining labs through your primary care provider, naturopathic doctor, or functional labs to assess hormone health, nutrient status, and inflammation.
Strengthen your foundations. Focus on the basics that matter most: eating nutrient-dense foods, prioritizing sleep, improving hydration, regulating stress, grounding your nervous system, and moving your body in ways that feel supportive rather than depleting.
Support your cycle with nutrition. Download our free handout on menstrual cycle–based meal ideas to learn how to nourish your body throughout each phase of your cycle.
Seek individualized care. Booking a session with us for pelvic floor physical therapy, bodywork, or pelvic health coaching can help you better understand your body, identify contributors to pain, and create a personalized plan forward.
Moving Forward
You don’t have to have everything figured out to start. Small, informed steps can create meaningful change, and your cycle is a powerful place to begin.
Start today, listen to your body, nourish it, and take the steps that feel right for you.