
Diastasis Recti Abdominis: Beyond the Gap

Diastasis Recti Abdominis—DRA—is one of the most common things people notice during and after pregnancy.
And the questions are almost always the same:
“Do I have a separation?”
“Are my abs supposed to come back together?”
“How big is the gap?”
“Will I need surgery?”
“Will my abs ever come back together?”
So let’s break this down in a way that actually makes sense—and hopefully bridge some of the gaps in how we talk about postpartum healing.
Do you have a separation?
Most likely, yes.
By the third trimester, nearly everyone develops some degree of separation through the abdominal wall. Your body is expanding to make space for a growing baby, and the connective tissue between your abdominal muscles stretches to allow that to happen.
That’s not a problem.
That’s expected.
So postpartum, if you’re feeling a gap, noticing a change in your abdomen, or feeling less supported—that’s a very normal place to start and you are not alone in that.
What is actually separating?
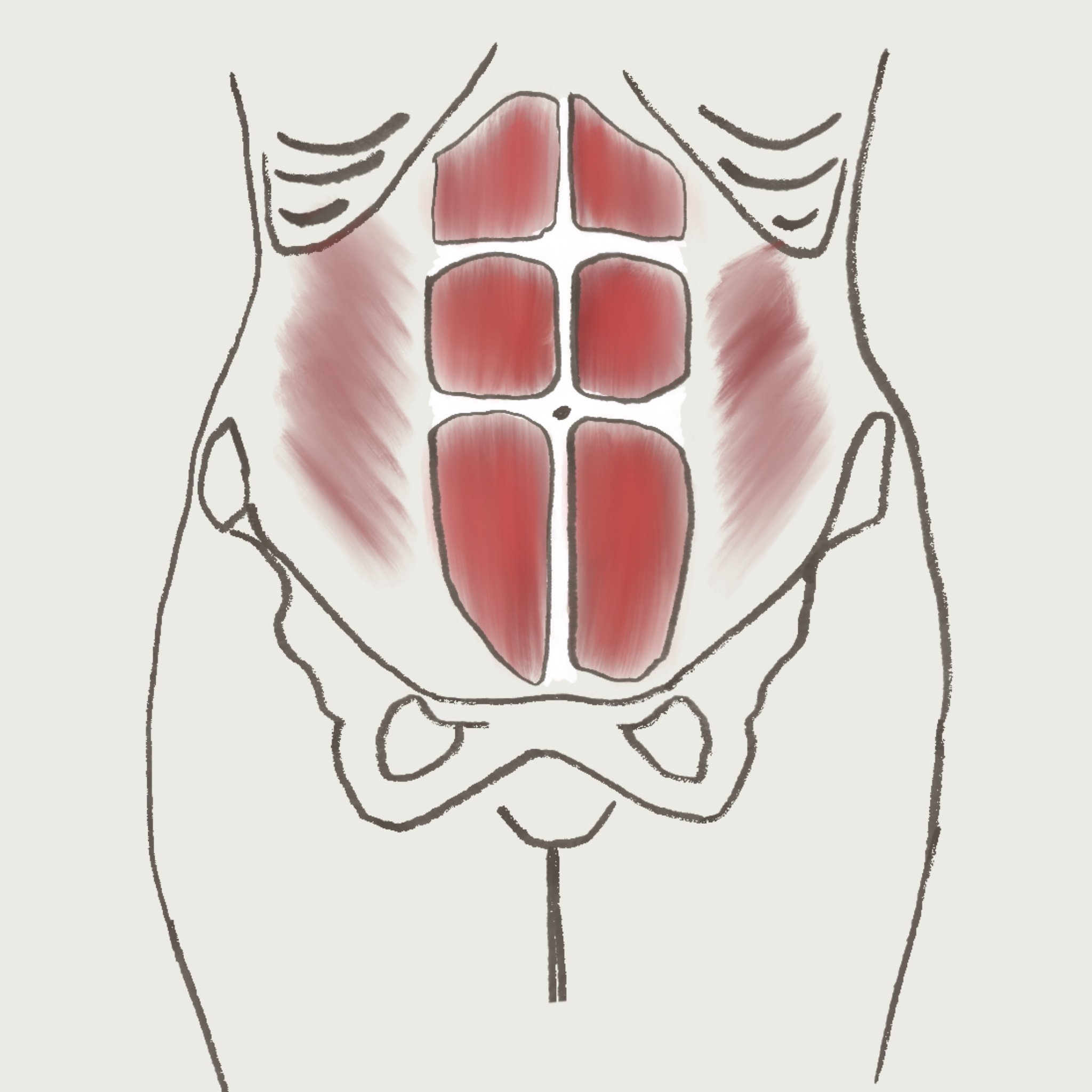
the rectus abdominus
You have two long muscles on the front of your abdomen—your rectus abdominis.
Between them is a band of connective tissue called the linea alba.
This connective tissue is meant to transfer force, create tension, and support your body when you move and lift.
During pregnancy, it stretches.
After pregnancy, it doesn’t just need to come back together—it needs to function well under load again too.
So yes—the gap matters… but not in the way you think
Most conversations stop at: “How wide is it?” And while width gives us information—it’s not the most important piece.
What really matters is how well that tissue can create tension to move and to function optimally.
Can you Assess Yourself for DRA?
Before you attempt to change anything or introduce anything new, we want to understand what’s going on with your body. Let’s walk through how you can check yourself at home.
Lie on your back, knees bent
Place fingers along your linea alba (midline):
at your belly button
2” above belly button
4” above belly button
6” above belly button
2” below belly button
4” below belly button
6” below belly button
Gently lift your head and shoulders at each placement
Feel for width and depth:
Width (the width from right side to your left side abdominal muscles
Depth aka “End-Feels” (how much can your fingers sink in”
Here we’re just gathering measurements to understand your body and it’s current functional capacity.
End-feels: what your fingers are actually telling you
When you check your DRA, what you feel matters just as much as what you measure.
Firm end-feel:
Your fingers meet resistance. The tissue pushes back.
→ This is what we want. It’s tension, support, and good load transfer.Semi-firm end-feel:
There’s some give on the midline (linea alba) but still some support.
→ This is okay. It just means there’s room to build more strength.Soft end-feel:
Your fingers sink in on the midline (linea alba) and there’s very little resistance.
→ This is where we need to work. The system isn’t generating enough tension yet.
So a measurement reading may look like this:
At belly button: 2.5” width, soft end feel
2” above belly button: 2.5” width, soft end feel
4” above belly button: 2” width, semi-firm end feel
6” above belly button: 1” width, firm end feel
2” below belly button: 2” width, semi-firm end feel
4” below belly button: 2” width, firm end feel
6: below belly button: 1” width, firm end feel
The importance of Width vs Depth (think: bridge, not gap)
Think of your abdominal wall like a bridge.
For example, you can have:
a wide bridge (a wide DRA) with strong suspension (firmness on the linea alba) → stable, supportive, handles load well
a narrow bridge (a narrow DRA) with poor support (softness on the linea alba) → wobbly, unstable, struggles under load
That’s the difference between width and depth/tension.
Width = how far apart the muscles are
Depth = how much tension the tissue can create
So you can have:
a wider gap that feels firm and supportive → good function
a smaller gap that feels soft and sinks in → needs work
Why this actually matters
Your core is not just your abs. It’s a system made up of your diaphragm, abdominal wall, pelvic floor, and back muscles. The core manages pressure, supports your spine, and transfers force when you move to provide stability. If this system isn’t working well, you might notice doming, low back discomfort, and other symptoms of DRA.
So instead of only asking: “How big is my gap?” We start asking: “Can my system handle load?”
This question is indicative of your end-feel tension.
Where Things Change: Loading the Muscles
This is where a lot of people get stuck. They either don’t load the system with enough, or push way past control.
We don’t want you doing either. Instead, the goal is to progressively load the system with appropriate movement strategies.
Current research supports progressive exercise that trains both deep and superficial abdominal muscles, combined with breathing and functional movement. Avoiding these strategies may make things worse.
Below, we’ve included a few exercises you can be doing for DRA, though each stage of your postpartum journey.
Early postpartum (first 6-12 weeks)
Focus on reconnecting:
Breath connection between diaphragm, abdominals, and pelvic floor muscles
gentle tensioning exercise
Coordination with the core muscles and movement strategies
Examples:
breathing with long exhale
heel slides
supported marching
light bridges
We’re teaching the system how to turn on again.
3–6 months Postpartum
Now we build from our foundation from exercises like:
dead bugs
bird dogs
Planks and side planks (modified if needed)
Weighted carries
squats and hinges
Now we care about:
maintaining tension
controlling pressure
not pushing through doming
Yes—even things like crunches can be appropriate if you can control pressure and tension.
6+ months Postpartum
Time to get stronger.
loaded carries
Core and plank progressions
rotational work
lifting
controlled abdominal strengthening
18+ months Postpartum
At this point, if things aren’t improving—it’s usually not about time.
It’s about how the system has (or hasn’t) been trained under tension.
This phase should look like real strength training and real life with professional support:
lifting
impact (if appropriate)
dynamic movement
full return to activity
The Myth of Exercise: Let’s Clear This Up
“Should I work out while pregnant?”
Yes, in most cases! Movement is beneficial. It’s about modifying where needed—not avoiding.
“Are crunches bad?”
Not automatically. It depends on control and pressure management, not the exercise itself.
“Should I avoid lifting?”
Long-term avoidance is not the goal. Learning how to manage pressure while lifting is.
What makes DRA worse — and What Makes it Better
Underloading our core system (not giving it much to work with), holding our breath, (and bearing down while holding the breath), and pushing through a workout when there’s poor control all make DRA worse.
Intentional, mindful movement; proper breath mechanics and progressive loading during a workout all help DRA improve. Training the whole system with intention, and not pushing past your limits, are always a good standard to have when we talk about DRA.
Surgery: What to Consider
Surgery for diastasis recti sometimes gets a bad rap, as if you’re not allowed to care about your body’s function or how you feel inside of it. Not only is this an unfair picture of surgery, but it also takes away your choice. It is fully your decision, no guilt involved, as to whether or not you go the surgery route.
No matter what you decide, we’re here to help with rehab!
Post-Surgical Rehab
When you’ve found a surgeon who cares for both function and aesthetic, it’s also important to find a pelvic therapy clinic that can help rehab your abdomen after surgery. Together, we’ll do lymphatic work, scar tissue mobilization, retrain your pressure mechanics, and work on progressive loading and return to fitness.
Surgery changes the structure, and you train the system.
Final thoughts
Where we start by thinking “I want to close this gap,” we hope that together we can work to restore the system that handles pressure, supports our spine, and distributes load.
Give yourself grace as you relearn your body after such a major life and body transition.
No matter where you’re at in this process, we’re here to support you. Check out our postpartum services, or book your free 15-minute consultation now!
Medical Disclaimer:
This blog is for educational purposes only and is not intended to replace medical advice, diagnosis, or treatment. Every body and situation is different—if you have specific concerns, symptoms, or questions, we recommend working with a licensed healthcare provider or pelvic health specialist.